L9 Part2 Reward
九、Reward
Reward refers to the positive effect an object or a condition—such as a drug, food, sexual contact, or warmth—has on the user.
Reward is accompanied by a tendency to repeat the behavior that brought about the reward and, typically, by feelings of pleasure.
The most important reward circuit is the mesolimbic pathway, which consists of dopaminergic neurons originating in the ventral tegmental area and connecting to several targets in the limbic system, especially the nucleus accumbens.
Microdialysis studies show that natural rewards—food, water, and sexual stimulation—increase dopamine levels in the nucleus accumbens of rats.
Other structures also participate in reward, including the amygdala, the hippocampus, the hypothalamus, and parts of the frontal cortex.
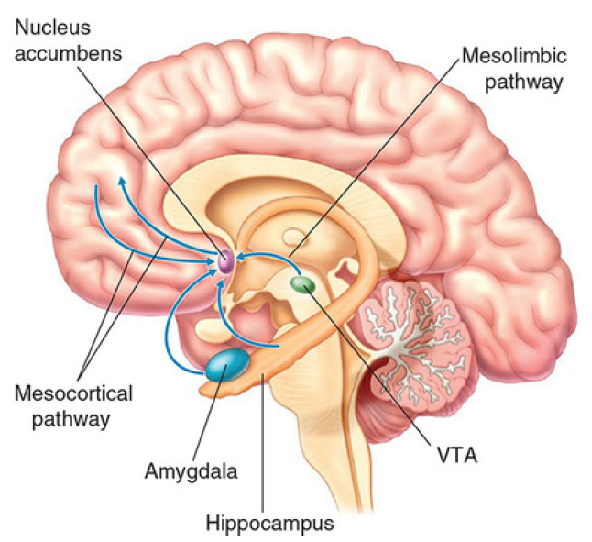
The mesolimbic system (中脑边缘系统) projects from dopamin(DA) neurons in the ventral tegmental area(VTA) to the nucleus accumbens;
The mesocortical system(中脑皮层系统) projects from DA neuons in the VTA to the frontal cortex.
Together, they form the mesolimbocortical dopamines system(中脑皮层多巴胺系统), so named becaus it begins in the midbrain(mesencephalon) and projects to the limblic system and prefrontal cortex.
In electrical stimulation of the brain (ESB), animals and, sometimes, humans learn to press a lever to deliver mild electrical stimulation to brain areas where the stimulation is rewarding.
- ESB is thought to reflect “natural” reward processes because, for example, effective sites are often in areas where experimenter-delivered stimulation evokes eating or sexual activity.
- However, ESB has a much more powerful effect than natural rewards. Animals will ignore food and water and tolerate painful shock to stimulate their brains with electricity, sometimes pressing a lever thousands of times in an hour.
Drugs are similarly powerful: Humans will sacrifice their careers, relationships, and lives in the interest of acquiring and using drugs. While food and sex increase dopamine in the nucleus accumbens by 50%–100%, drugs and electrical stimulation can have a three- to sixfold greater effect.
Reward and Addiction
Rats will learn to press a lever to inject abused drugs, and lesioning the nucleus accumbens(伏隔核) reduces reward effects for many drugs.
All abused drugs target the mesolimbic dopamine system and increase dopaminergic activity.
If dopamine activity is blocked, rats will not learn to press a lever for a drug injection, and those that have learned previously will stop lever pressing after receiving the dopamine-blocking drug.
In PET scan studies, human volunteers who had the greatest increase in dopamine in the general area of the nucleus accumbens during drug administration also experienced the most intense “highs”.
In one study, participants began reporting that they felt “high” when cocaine had blocked 47% of the dopamine reuptake sites in the nucleus accumbens.
1. Drug Addiction
What Is Addiction?
- The term addiction derives from the Latin word addicere, “to sentence.”
- Someone who is addicted to a drug is, in a way, sentenced to a term of involuntary servitude, being obliged to fulfill the demands of his or her drug dependency.
Drug addiction poses a serious problem to our species.
Consider the disastrous effects caused by the abuse of one of our oldest drugs, alcohol: automobile accidents, fetal alcohol syndrome, cirrhosis of the liver, Korsakoff’s syndrome, increased rate of heart disease, and increased rate of intracerebral hemorrhage.
- Smoking (addiction to nicotine) greatly increases the chances of dying of lung cancer, heart attack, and stroke; and women who smoke give birth to smaller, less healthy babies.
- Cocaine addiction can cause psychotic behavior, brain damage, and death from overdose; and competition for lucrative and illegal markets terrorizes neighborhoods, subverts political and judicial systems, and causes many violent deaths.
The use of “designer drugs” exposes users to unknown dangers of untested and often contaminated products, as several people discovered when they acquired Parkinson’s disease after taking a synthetic opiate that was tainted with a neurotoxin.
Addicts who take their drugs intravenously run a serious risk of contracting AIDS, hepatitis, or other infectious diseases.
2. A Little Background
Long ago, people discovered that many substances found in nature—primarily leaves, seeds, and roots of plants but also some animal products—had medicinal qualities.
They discovered herbs that helped to prevent infections, that promoted healing, that calmed an upset stomach, that reduced pain, or that helped to provide a night’s sleep.
They also discovered “recreational drugs”—drugs that produced pleasurable effects when eaten, drunk, or smoked.
The most universal recreational drug, and perhaps the first one that our ancestors discovered, is ethyl alcohol. Yeast spores are present everywhere, and these microorganisms can feed on sugar solutions and produce alcohol as a by-product. Undoubtedly, people in many different parts of the world discovered the pleasurable effects of drinking liquids that had been left alone for a while, such as the juice that had accumulated in the bottom of a container of fruit.
3. Addictive Drugs
| Drug | Sites of Action |
|---|---|
| Ethyl alcohol | NMDA receptor (indirect antagonist); GABAA receptor(indirect agonist) |
| Barbiturates 巴比妥酸盐 | GABAA receptor (indirect agonist) |
| Benzodiazepines (tranquilizers) 苯二氮卓类 | GABAA receptor (indirect agonist) |
| Cannabis (marijuana) 大麻 | CB1 cannabinoid receptor (agonist) |
| Nicotine | Nicotinic ACh receptor (agonist) |
| Opiates (heroin, morphine, etc.) 阿片类 | μ and δ opiate receptor agonist |
| Phencyclidine (PCP) and ketamine 苯环啶和氯胺酮 | NMDA receptor (indirect antagonist) |
| Cocaine | Blocks reuptake of dopamine (and serotonin andnorepinephrine) |
| Amphetamine 安非他命/苯丙胺 | Causes release of dopamine (by running dopaminetransporters in reverse) |
4. Addiction: Positive Reinforcement
Drugs that lead to dependency must first reinforce people’s behavior.
- Positive reinforcement refers to the effect that certain stimuli have on the behaviors that preceded them. If, in a particular situation, a behavior is regularly followed by an appetitive stimulus (one that the organism will tend to approach), then that behavior will become more frequent in that situation.
- The effectiveness of a reinforcing stimulus is greatest if it occurs immediately after a response occurs.
- If the reinforcing stimulus is delayed, it becomes considerably less effective.
Drug users prefer heroin to morphine, because it has a more rapid effect.
- In fact, heroin is converted to morphine as soon as it reaches the brain. But because heroin is more lipid soluble, it passes through the blood–brain barrier more rapidly, and its effects on the brain are felt sooner than those of morphine.
- The most potent reinforcement occurs when drugs produce sudden changes in the activity of the reinforcement mechanism; slow changes are much less reinforcing. A person taking an addictive drug seeks a sudden “rush” produced by a fast-acting drug.
- The reason for this fact is found by examining the function of instrumental (operant) conditioning: learning about the consequences of their own behavior.
- Normally, causes and effects are closely related in time; we do something, and something happens, good or bad. The consequences of the actions teach us whether to repeat that action, and events that follow a response by more than a few seconds were probably not caused by that response.
- All natural reinforcers that have been studied so far (such as food for a hungry animal, water for a thirsty one, or sexual contact) have one physiological effect in common: They cause the release of dopamine in the nucleus accumbens (White, 1996).
Addictive drugs—including amphetamine, cocaine, opiates, nicotine, alcohol, PCP, and cannabis—trigger the release of dopamine in the nucleus accumbens, as measured by microdialysis (Di Chiara, 1995).
Different drugs stimulate the release of dopamine in different ways.
- The fact that the reinforcing properties of addictive drugs involve the same brain mechanisms as natural reinforcers indicated that these drugs “hijack” brain mechanisms that normally help us adapt to our environment.
- It appears that the process of addiction begins in the mesolimbic dopaminergic system and then produces long-term changes in other brain regions that receive input from these neurons (Kauer and Malenka, 2007).
The first changes appear to take place in the ventral tegmental area (VTA). A single administration of a variety of addictive drugs (including cocaine, amphetamine, morphine, alcohol, and nicotine) increased the strength of excitatory synapses on dopaminergic neurons in the VTA in mice.
This change appeared to result from insertion of additional AMPA receptors into the postsynaptic membrane of the DA neurons (Mameli et al., 2009). This process, normally mediated by glutamatergic NMDA receptors, is the neural basis of many forms of learning. A single injection of an addictive drug produces synaptic strengthening in the VTA that lasts for about five days. If an animal receives cocaine for about two weeks, the changes in the VTA persist.
5. Addiction: Negative Reinforcement
An old joke
someone says that the reason he bangs his head against the wall is that “it feels so good when I stop
A behavior that turns off (or reduces) an aversive stimulus will be reinforced. This phenomenon is known as negative reinforcement.
Negative reinforcement
- The removal or reduction of an aversive stimulus that is contingent on a particular response, with an attendant increase in the frequency of that response.
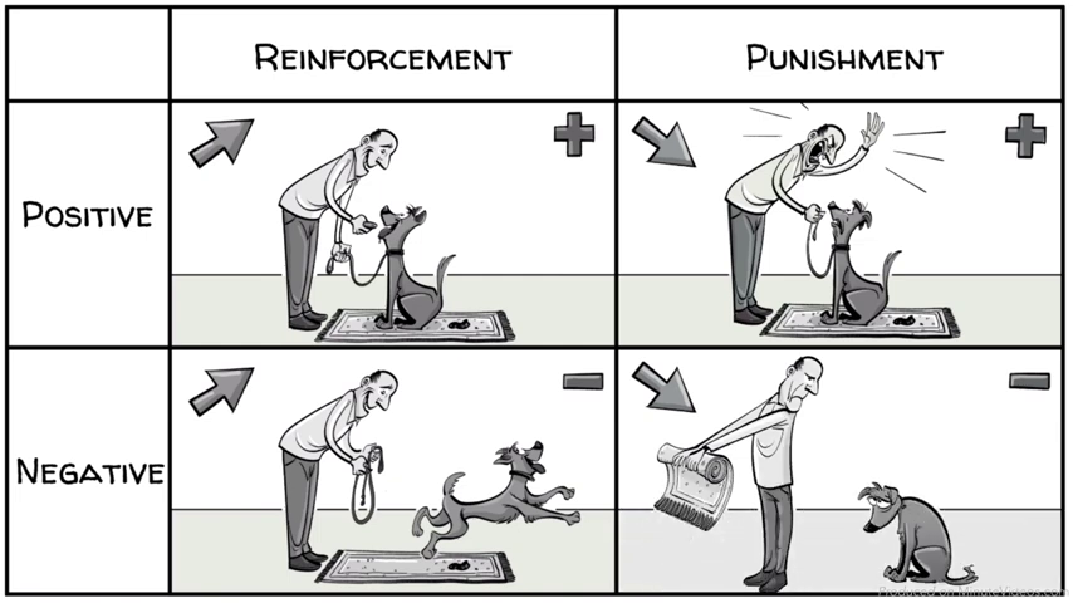
Reinforcement and Punishment
We can increase or decrease a behavior by adding a consequence. e.g. A dog poops on a carpet. We have four possible ways to teach the dog a lesson.
Positive reinforcement seems to be what provokes drug taking in the first place.
Negative reinforcement (reduction of withdrawal effects) could play a role in maintaining someone’s drug addiction. The withdrawal effects are unpleasant, but as soon as the person takes some of the drug, these effects go away, producing negative reinforcement.
Negative reinforcement could also explain the acquisition of drug addictions under some conditions. If a stressed person is suffering from some unpleasant feelings and then takes a drug that eliminates these feelings, the person’s drug-taking behavior is likely to be reinforced. For example, alcohol can relieve feelings of anxiety. If a person finds himself in a situation that arouses anxiety, he might find that having a drink or two makes him feel much better.
People who abuse some drugs become physically dependent on the drug; that is, they show tolerance and withdrawal symptoms.
Tolerance is the decreased sensitivity to a drug that comes from its continued use; a user must take larger and larger amounts of the drug for it to be effective.
Once a person has taken an opiate regularly enough to develop tolerance, that person will suffer withdrawal symptoms if he or she stops taking the drug.
Withdrawal symptoms are primarily the opposite of the effects of the drug itself. The effects of heroin—euphoria, constipation, and relaxation—lead to the withdrawal effects of dysphoria, cramping and diarrhea, and agitation.
Tolerance
- The fact that increasingly large doses of drugs must be taken to achieve a particular effect; caused by compensatory mechanisms that oppose the effect of the drug.
Withdrawal symptoms
- The appearance of symptoms opposite to those produced by a drug when the drug is suddenly no longer taken; caused by the presence of compensatory mechanisms.
Most investigators believe that tolerance is produced by the body’s attempt to compensate for the unusual condition of heroin intoxication.
- The drug disturbs normal homeostatic mechanisms in the brain, and in reaction these mechanisms begin to produce effects opposite to those of the drug, partially compensating for the disturbance.
Because of these compensatory mechanisms, the user must take increasing amounts of heroin to achieve the effects that were produced when he or she first started taking the drug. These mechanisms also account for the symptoms of withdrawal: When the person stops taking the drug, the compensatory mechanisms make themselves felt, unopposed by the action of the drug.
6. Addiction: Craving and Relapse
Why do drug addicts crave drugs? Why does this craving occur even after a long period of abstinence? Even after going for months or years without taking an addictive drug, a former drug addict might sometimes experience an intense craving that leads to relapse.
Clearly, taking a drug over an extended period of time must produce some long-lasting changes in the brain that increase a person’s likelihood of relapsing. Understanding this process might help clinicians to devise therapies that will assist people in breaking their drug dependence once and for all.
One of the ways in which craving has been investigated in laboratory animals is through the reinstatement model of drug seeking.
Animals are first trained to make a response (for example, pressing a lever) that is reinforced by intravenous injections of a drug such as cocaine. \
Next, the response is extinguished by providing injections of a saline solution rather than the drug.
Once the animal has stopped responding, the experimenter administers a “free” injection of the drug (drug reinstatement procedure) or presents a stimulus that has been associated with the drug (cue reinstatement procedure).
In response to these stimuli, the animals begin responding at the lever once more.
Presumably, this kind of relapse (reinstatement of a previously extinguished response) is a good model for the craving that motivates drug-seeking behavior in a former addict.
The Reinstatement Procedure, a Measure of Craving
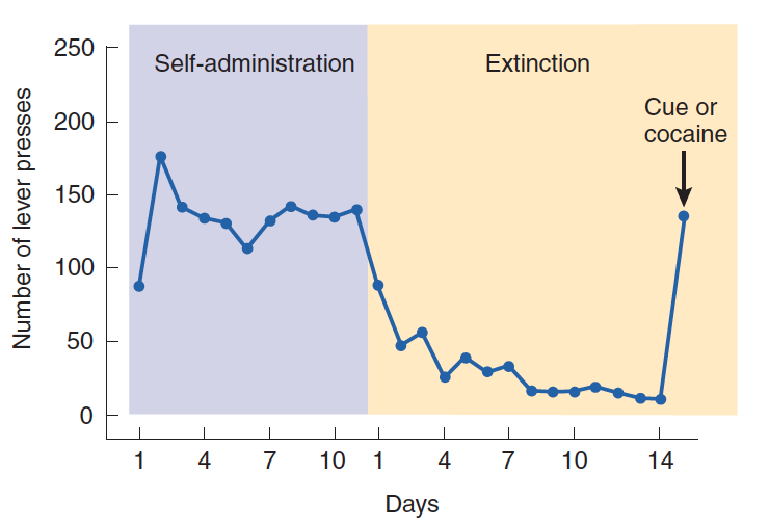
- The graph shows the acquisition of lever pressing for injections of an addictive drug during the self-administration phase, as well as the extinction of lever pressing when the drug was no longer administered. A “free” shot of the drug or presentation of a cue associated with the drug during acquisition will reinstate responding.
Role of prefrontal cortex
Ventromedial prefrontal cortex (vmPFC) is responsible for extinction of conditioned fear memory. Lesions of the vmPFC impair extinction.
- Ventromedial prefrontal cortex plays an important role in regulating our responses to situations in frustration. VmPFC plays a role in inhibiting emotional responses.
The prefrontal cortex plays a role in emotional reactions guide moral judgments and decisions involving personal risks and rewards.
- Whether prefrontal cortex involves in drug craving and repase?
Cocaine Intake and the Medial Prefrontal Cortex:
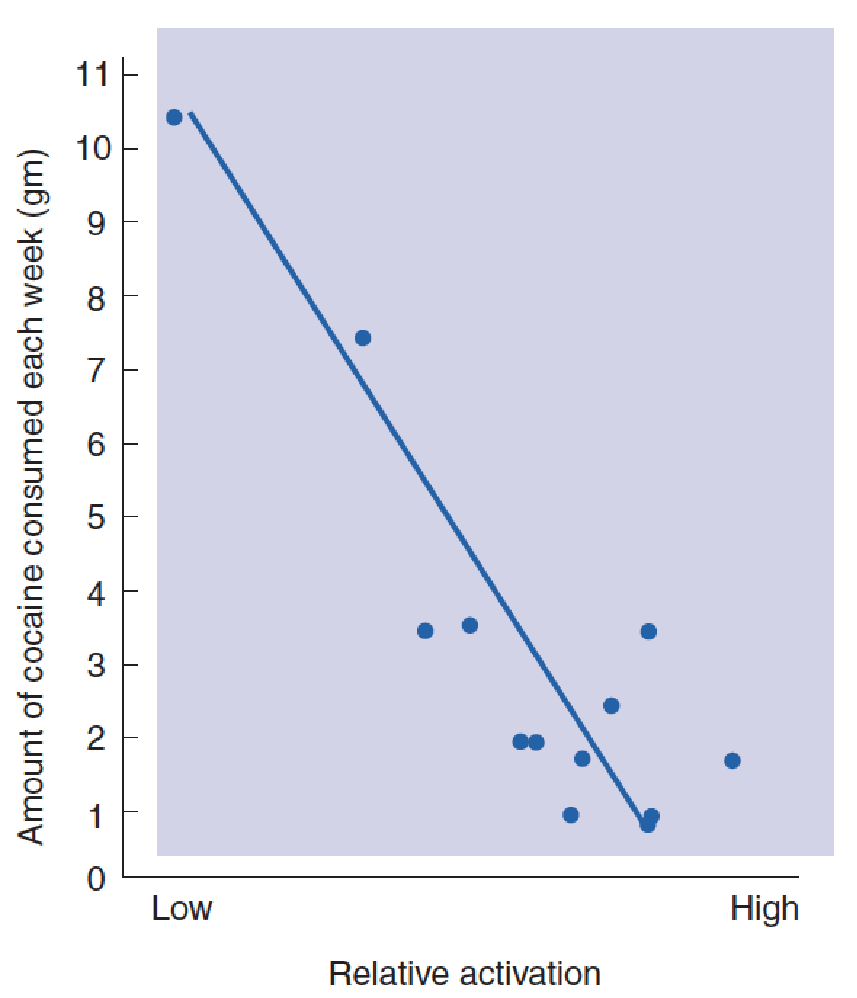
- The graph shows the relative activation of the medial prefrontal cortex as a function of the amount of cocaine normally taken each week by cocaine abusers.
Volkow et al. (2002) found that the activity of the medial prefrontal cortex of cocaine abusers was lower than that of normal subjects during abstinence.
- In addition, when addicts are performing tasks that normally activate the prefrontal cortex, their medial prefrontal cortex is less activated than that of healthy control subjects, and they perform more poorly on the tasks.
In fact, Bolla and her colleagues found that the amount of activation of the medial prefrontal cortex was inversely related to the amount of cocaine that cocaine abusers normally took each week: The lower the brain activity, the more cocaine the person took.
- People with a long history of drug abuse not only show the same deficits on tasks that involve the prefrontal cortex as do people with lesions of this region, they also show structural abnormalities of this region.
Franklin et al. (2002) reported an average decrease of 5–11% in the gray matter of various regions of the prefrontal cortex of chronic cocaine abusers.
de Ruiter et al. (2011) found evidence of loss of behavioral control caused by decreased activation of the dorsomedial PFC in both heavy smokers and pathological gamblers, which supports the assertion of some investigators that pathological gambling should be regarded as a form of addiction (Thomas et al., 2011).
Of course, the results of these studies do not permit us to determine whether abnormalities in the prefrontal cortex predispose people to become addicted or whether drug taking causes these abnormalities (or both).
Role of corticotropin-releasing hormone (CRH)
The presence of drug-related stimuli can trigger craving and drug-seeking behavior.
In addition, clinicians have long observed that stressful situations can cause former drug addicts to relapse.
- These effects have also been observed in rats that had previously learned to self-administer cocaine or heroin (Covington and Miczek, 2001).
The mechanism that triggers relapse appears to involve the stress-induced release of corticotropin-releasing hormone (CRH) in the brain.
A study by Hahn, Hopf, and Bonci (2009) found that infusion of CRH caused an enhanced activation of dopaminergic neurons in the ventral tegmental area in mice that had been exposed to cocaine.
Commonly Abused Drugs
1. Opiates 鸦片;阿片类
Opium, derived from the opium poppy, has been eaten and smoked for centuries.
The most commonly abused opiate is heroin.
Opiate addiction has several high personal and social costs.
- First, heroin is an illegal drug in most countries, an addict becomes a criminal.
- Second, because of tolerance, a person must take increasing amounts of the drug to achieve a “high.” The habit thus becomes more and more expensive, and the person often turns to crime to obtain enough money to support his or her habit.
- Third, an opiate addict often uses unsanitary needles; at present, a substantial percentage of people who inject illicit drugs have been exposed in this way to hepatitis or the AIDS virus.
- Fourth, if the addict is a pregnant woman, her infant will also become dependent on the drug, which easily crosses the placental barrier. The infant must be given opiates right after being born and then weaned off the drug with gradually decreasing doses.
- Fifth, the uncertainty about the strength of a given batch of heroin makes it possible for a user to receive an unusually large dose of the drug, with possibly fatal consequences. And some of the substances used to dilute heroin are themselves toxic.
When an opiate is administered systemically, it stimulates opiate receptors located on neurons in various parts of the brain and produces a variety of effects, including analgesia, hypothermia (lowering of body temperature), sedation, and reinforcement.
- Opiate receptors in the periaqueductal gray matter are primarily responsible for the analgesia,
- those in the preoptic area are responsible for the hypothermia,
- those in the mesencephalic reticular formation are responsible for the sedation,
- those in the ventral tegmental area (VTA) and the nucleus accumbens (NAC) are responsible for the reinforcing effects of opiates.
Injections of opiates cause the release of dopamine in the NAC. The level of dopamine in the NAC increased by 150 – 300% while a rat was pressing a lever that delivered intravenous injections of heroin.
2. Stimulant Drugs: Cocaine and Amphetamine
Cocaine and amphetamine have similar behavioral effects, because both act as potent dopamine agonists.
- However, their sites of action are different.
Cocaine binds with and deactivates the dopamine transporter proteins, thus blocking the reuptake of dopamine after it is released by the terminal buttons.
Amphetamine also inhibits the reuptake of dopamine, but its most important effect is to directly stimulate the release of dopamine from terminal buttons.
- Methamphetamine is chemically related to amphetamine, but is considerably more potent.
Because the effects of cocaine and methamphetamine are so potent and so rapid, they are probably the most effective reinforcers of all available drugs.
In fact, if rats or monkeys are given continuous access to a lever that permits them to self-administer cocaine, they often self-inject so much cocaine that they die.
Rats that self-administered cocaine were almost three times more likely to die than rats that self-administered heroin
Some evidence suggests that the use of stimulant drugs may have adverse long-term effects on the brain.
A PET study discovered that prior abusers of methamphetamine showed a decrease in the numbers of dopamine transporters in the caudate nucleus and putamen, despite the fact that they had abstained from the drug for approximately three years. The decreased number of dopamine transporters suggests that the number of dopaminergic terminals in these regions is diminished. These people might have an increased risk of Parkinson’s disease as they get older.
Dopamine Transporters, Methamphetamine Abuse, and Parkinson’s Disease:
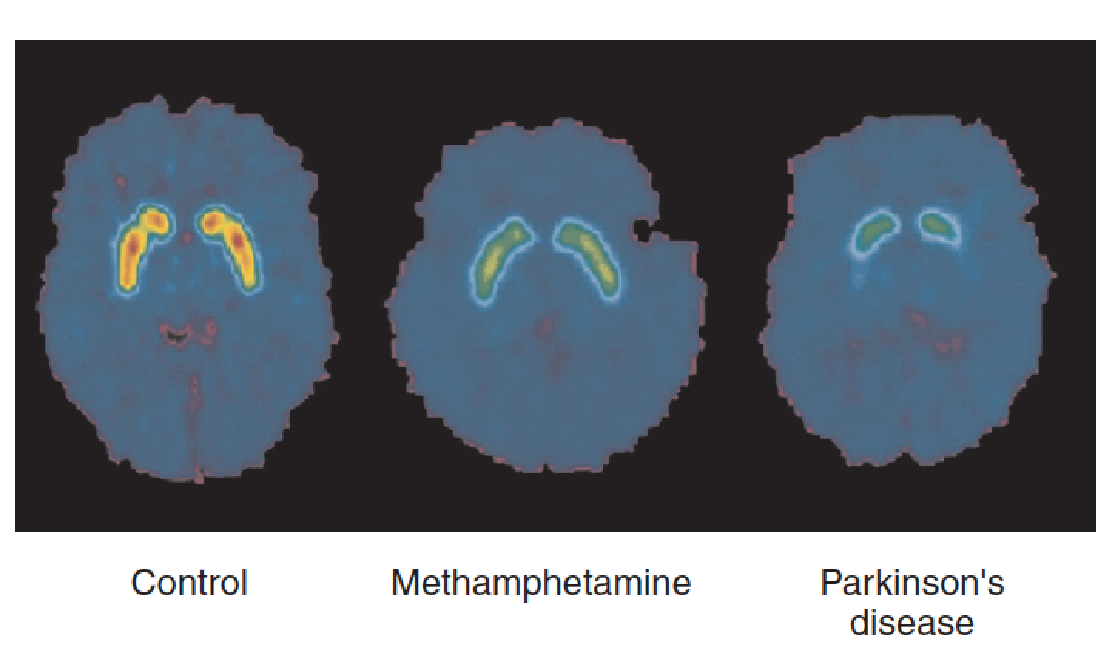
- The scans show concentrations of dopamine transporters from a control subject, a subject who had previously abused methamphetamine, and a subject with Parkinson’s disease. Decreased concentrations of dopamine transporters indicate loss of dopaminergic terminals.
3. Nicotine
Nicotine might seem rather tame in comparison to opiates, cocaine, and amphetamine. Nevertheless, nicotine is an addictive drug, and it accounts for more deaths than the so-called “hard” drugs.
The combination of nicotine and other substances in tobacco smoke is carcinogenic and leads to cancer of the lungs, mouth, throat, and esophagus.
Approximately one-third of the adult population of the world smokes, and smoking is one of the few causes of death that is rising in developing countries.
Smoking by pregnant women also has negative effects on the health of their fetuses—apparently worse than those of cocaine. Unfortunately, approximately 25 percent of pregnant women in the United States expose their fetuses to nicotine.
Ours is not the only species willing to self-administer nicotine; so will laboratory animals.
Nicotine stimulates nicotinic acetylcholine receptors. It also increases the activity of dopaminergic neurons of the mesolimbic system and causes dopamine to be released in the NAC.
Nicotine and Dopamine Release in the Nucleus Accumbens:
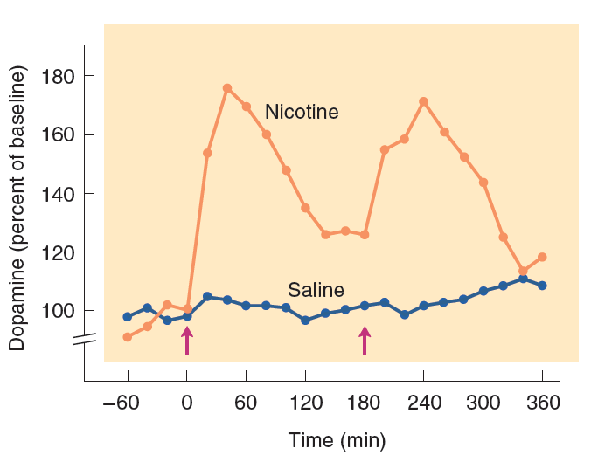
- The graph shows changes in dopamine concentration in the nucleus accumbens, measured by microdialysis, in response to injections of nicotine or saline. The arrows indicate the time of the injections.
Studies have found that the endogenous cannabinoids play a role in the reinforcing effects of nicotine.
Rimonabant, a drug that blocks cannabinoid CB1 receptors, blocks the reinforcing effects of nicotine in rats, apparently by reducing the release of dopamine in the NAC.
Rimonabant has been used to help prevent relapse in people who are trying to quit smoking.
Insular damage also lost the urge to smoke.
Naqvi and his colleagues (2007) identified nineteen cigarette smokers with damage to the insula and fifty smokers with brain damage that spared this region. Nineteen of the patients had damage to the insula, and twelve of them “quit smoking easily, immediately, without relapse, and without persistence of the urge to smoke”. One patient with insular damage quit smoking but still reported feeling an urge to smoke.
Damage to the Insula and Smoking Cessation:
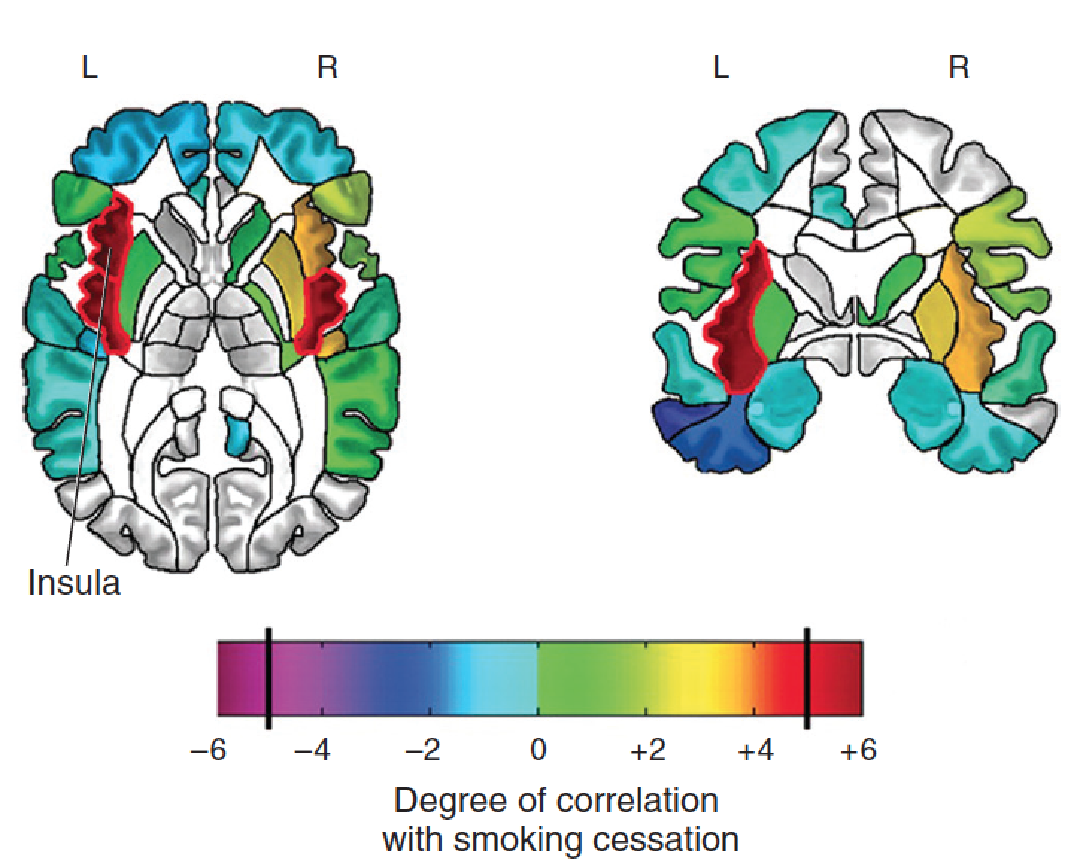
- The diagrams show the regions of the brain (shown in red) where damage was most highly correlated with cessation of smoking.
Infusion of an inhibitory drug into the insula of rats reduced the reinforcing effects of nicotine.
Investigators also found that the insula was larger in smokers, which is consistent with the apparent role of the insula in nicotine addiction.
Effect of Inactivation of the Insula on Reinstatement of Drug-Seeking Behavior in Rats:
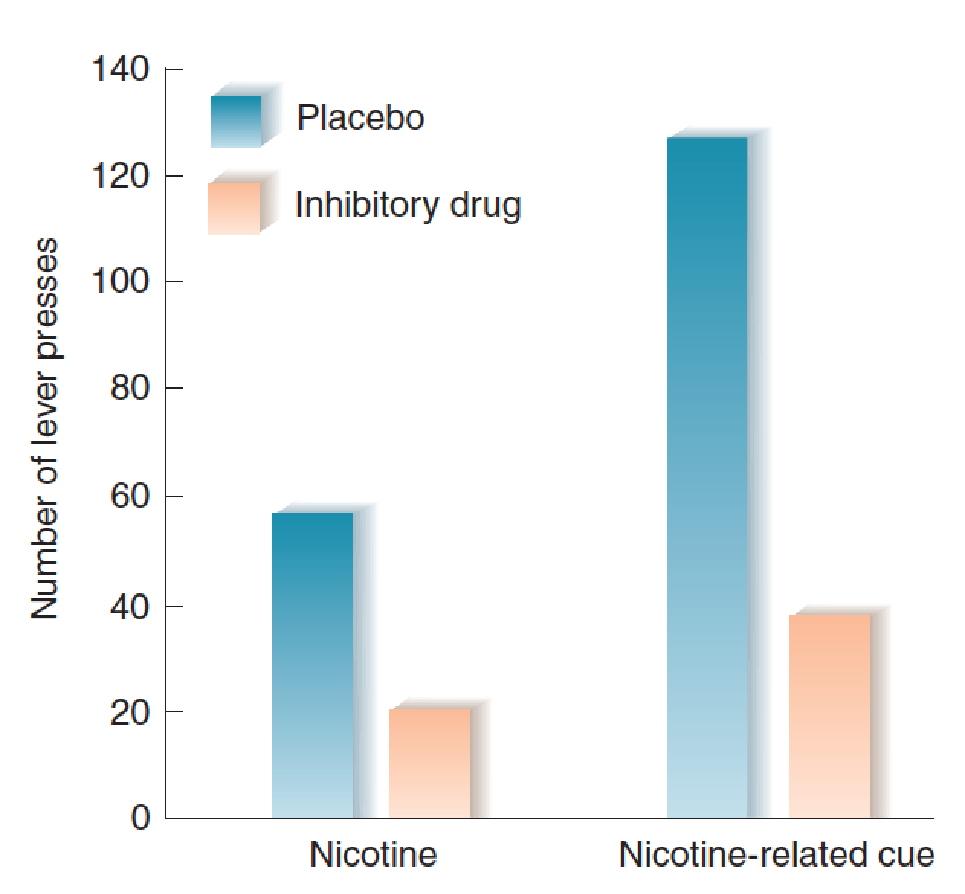
- Rats were trained to work for injections of nicotine, and then the behavior was extinguished. The graph shows that inactivation of the insula with an inhibitory drug substantially reduced drug-seeking behavior elicited by nicotine or cues previously associated with nicotine.
One of the several deterrents to cessation of smoking is the fact that overeating and weight gain frequently occur when people stop smoking.
Eating and a reduction in metabolic rate are stimulated by the release of MCH and orexin in the brain.
Nicotine inhibits MCH neurons, thus suppressing appetite. When people try to quit smoking, they are often discouraged by the fact that the absence of nicotine in their brains releases their MCH neurons from this inhibition, increasing their appetite.
Nicotine also stimulates the release of orexin, which is involved in drug-seeking behavior (Huang, Xu, and van den Pol, 2011). Orexin is released in many parts of the brain, but one region may play an especially important role in smoking: the insula. Hollander et al. (2008) found that infusion of a drug into the insula that blocks orexin receptors decreased the responding of rats for injections of nicotine.
4. Alcohol
Alcohol has enormous costs to society.
- A large percentage of deaths and injuries caused by motor vehicle accidents are related to alcohol use.
- Alcohol contributes to violence and aggression.
- Chronic alcoholics often lose their jobs, their homes, and their families; and many die of cirrhosis of the liver, exposure, or diseases caused by poor living conditions and abuse of their bodies.
- Women who drink during pregnancy run the risk of giving birth to babies with fetal alcohol syndrome, which includes malformation of the head and the brain and accompanying mental retardation.
Therefore, understanding the physiological and behavioral effects of this drug is an important issue.
- At low doses, alcohol produces mild euphoria and has an anxiolytic effect—that is, it reduces the discomfort of anxiety.
- At higher doses, it produces incoordination and sedation.
In studies with laboratory animals, the anxiolytic effects manifest themselves as a release from the punishing effects of aversive stimuli.
For example, if an animal is given electric shocks whenever it makes a particular response (say, one that obtains food or water), it will stop doing so. However, if it is then given some alcohol, it will begin making the response again.
This phenomenon explains why people often do things they normally would not when they have had too much to drink; the alcohol removes the inhibitory effect of social controls on their behavior.
Alcohol, like other addictive drugs, increases the activity of the dopaminergic neurons of the mesolimbic system and increases the release of dopamine in the NAC as measured by microdialysis.
An injection of a dopamine antagonist directly into the NAC decreases alcohol intake, as does the injection of a drug into the VTA that decreases the activity of the dopaminergic neurons there.
Alcohol has two major sites of action in the nervous system, acting as an indirect antagonist at NMDA receptors and an indirect agonist at GABAA receptors.
That is, alcohol enhances the action of GABA at GABAA receptors and interferes with the transmission of glutamate at NMDA receptors.
The anxiolytic effects of a GABAA agonist are apparently responsible for the negatively reinforcing effects of alcohol.
The sedative effect of alcohol also appears to be exerted at the GABAA receptor.
Suzdak et al. (1986) discovered a drug (Ro15–4513) that reverses alcohol intoxication by blocking the alcohol binding site on this receptor.
Effects of Ro15–4513, an Alcohol Antagonist:
- Both rats received an injection of alcohol, but the one facing us also received an injection of the alcohol antagonist
This wonder drug has not been put on the market, nor is it likely to be. Although the behavioral effects of alcohol are mediated by their action on GABAA receptors and NMDA receptors, high doses of alcohol have other, potentially fatal effects on all cells of the body, including destabilization of cell membranes. Thus, people taking some of the alcohol antagonist could then go on to drink themselves to death without becoming drunk in the process. Drug companies naturally fear possible liability suits stemming from such occurrences.

The effects of alcohol withdrawal are serious and can even be fatal.
The increased sensitivity of NMDA receptors as they rebound from the suppressive effect of alcohol can trigger seizures and convulsions.
Convulsions caused by alcohol withdrawal are considered to be a medical emergency and are usually treated with an intravenous injection of a benzodiazepine.
Liljequist (1991) found that seizures caused by alcohol withdrawal could be prevented by giving mice a drug that blocks NMDA receptors.
As mentioned earlier that opiate receptors appear to be involved in a reinforcement mechanism that does not directly involve dopaminergic neurons. The reinforcing effect of alcohol is at least partly caused by its ability to trigger the release of the **endogenous opioids. **
Drugs that block opiate receptors also block the reinforcing effects of alcohol.
In addition, endogenous opioids may play a role in craving among abstinent alcoholics.
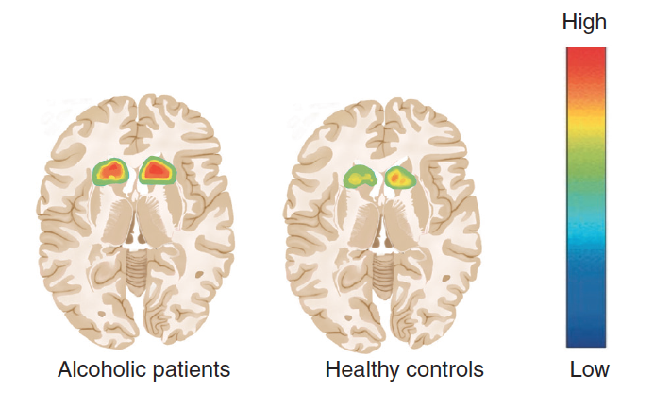
Heinz et al. (2005) found that one to three weeks of abstinence increased the number of μ opiate receptors in the NAC.
The greater the number of receptors, the more intense the craving was. Presumably, the increased number of μ receptors increased the effects of endogenous opiates on the brain and served as a contributing factor to the craving for alcohol.
Craving for Alcohol and μ Opiate Receptors:
- The PET scans show the presence of μ opiate receptors in the dorsal striatum of detoxified alcoholic patients and healthy control subjects.
5. Cannabis 大麻
Another drug that people regularly self-administer—almost exclusively by smoking—is THC(四氧大麻酚), the active ingredient in marijuana.
The site of action of the endogenous cannabinoids in the brain is the CB1 receptor. Administration of a drug that blocks CB1 receptors abolishes the “high” produced by smoking marijuana.
THC, like other drugs with abuse potential, has a stimulating effect on dopaminergic neurons.
THC and Dopamine Secretion in the Nucleus Accumbens :
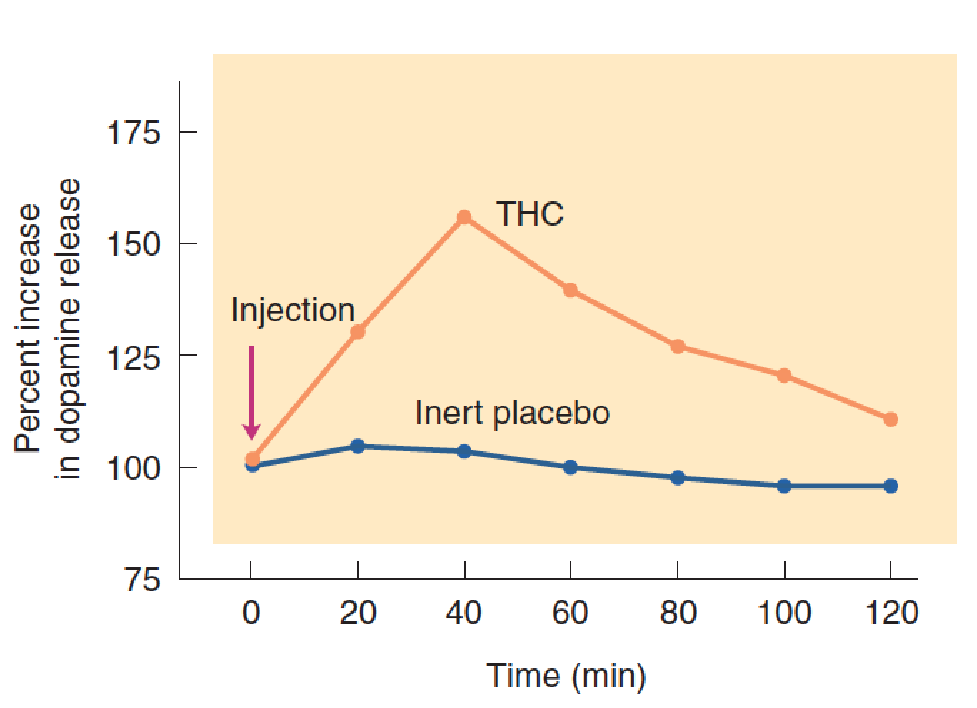
- The graph shows changes in dopamine concentration in the nucleus accumbens, measured by microdialysis, in response to injections of THC or an inert placebo.
The primary reinforcing component of marijuana, THC, is one of approximately seventy different chemicals produced only by the cannabis plant.
Another chemical, cannabidiol (CBD), plays an entirely different role.
Unlike THC, which produces anxiety and psychotic-like behavior in large doses, CBD has antianxiety and antipsychotic effects.
- THC is a partial agonist of cannabinoid receptors, whereas CBD is an antagonist.
Also unlike THC, CBD does not produce psychotropic effects: It is not reinforcing, and it does not produce a “high.”
The hippocampus contains a large concentration of THC receptors. Marijuana is known to affect people’s memory. Specifically, it impairs their ability to keep track of a particular topic; they frequently lose the thread of a conversation if they are momentarily distracted. Evidence indicates that the drug does so by disrupting the normal functions of the hippocampus, which plays such an important role in memory (Kunos and Batkai, 2001).
Heredity and Drug Abuse
Not everyone is equally likely to become addicted to a drug.
Many people manage to drink alcohol moderately, and most users of potent drugs such as cocaine and heroin use them “recreationally” without becoming dependent on them.
Evidence indicates that both genetic and environmental factors play a role in determining a person’s likelihood of consuming drugs and of becoming dependent on them.
In addition, there are both general factors (likelihood of taking and becoming addicted to any of a number of drugs) and specific factors (likelihood of taking and becoming addicted to a particular drug).
Therapy for Drug Abuse
There are many reasons for engaging in research on the physiology of drug abuse, including an academic interest in the nature of reinforcement and the pharmacology of psychoactive drugs.
But most researchers entertain the hope that the results of their research will contribute to the development of ways to treat and (better yet) prevent drug abuse in members of our own species.
As you well know, the incidence of drug abuse is far too high, so obviously, research has not yet solved the problem. However, real progress is being made.
The most common treatment for opiate addiction is methadone maintenance.
Methadone is a potent opiate, just like morphine or heroin. If it were available in a form suitable for injection, it would be abused.
Methadone maintenance programs administer the drug to their patients in the form of a liquid, which they must drink in the presence of the personnel supervising this procedure. Because the oral route of administration increases the opiate level in the brain slowly, the drug does not produce a high, the way an injection of heroin will. In addition, because methadone is long-lasting, the patient’s opiate receptors remain occupied for a long time, which means that an injection of heroin has little effect. Of course, a very large dose of heroin will still produce a “rush,” so the method is not foolproof.
A newer drug, buprenorphine, shows promise of being an even better therapeutic agent for opiate addiction than methadone (Vocci, Acri, and Elkashef, 2005).
Buprenorphine is a partial agonist for the μ opiate receptor. (A partial agonist is a drug that has a high affinity for a particular receptor but activates that receptor less than the normal ligand does. This action reduces the effects of a receptor ligand in regions of high concentration and increases it in regions of low concentration).
Buprenorphine blocks the effects of opiates and itself produces only a weak opiate effect. Unlike methadone, it has little value on the illicit drug market. The addition of a small dose of naloxone, a drug that blocks opiate receptors, ensures that the combination drug has no abuse potential—and will, in fact, cause withdrawal symptoms if it is taken by an addict who is currently taking an opiate. A major advantage of buprenorphine, besides its efficacy, is the fact that it can be used in office-based treatment.
An interesting approach to cocaine addiction was suggested from a study by Carrera et al. (1995), who conjugated cocaine to a foreign protein and managed to stimulate rats’ immune systems to develop antibodies to cocaine. The antibodies bound with molecules of cocaine and prevented them from crossing the blood–brain barrier. As a consequence, these “cocaine-immunized” rats were less sensitive to the activating effects of cocaine, and brain levels of cocaine in these animals were lower after an injection of cocaine.
Since this study was carried out, animal studies with vaccines against cocaine, heroin, methamphetamine, and nicotine have been carried out, and several human clinical trials with vaccines for cocaine and nicotine have taken place (Cerny and Cerny, 2009; Carroll et al., 2011; Hicks et al., 2011; Stowe et al., 2011).